Anesthesia, EEG versus CBF
Posted: Wed Mar 17, 2021 4:46 pm
Even after my debates on the previous incarnation of this forum I am still perplexed as to the dismissal of anesthesia as a thorn in the side of idealism by most debaters on this forum. Whilst I did state before in my previous post in this new forum that there is people under low doses of anesthesia whom act conscious whilst under whom do not remember a damn thing despite being conscious, thus the subject of memory becomes a big problem for an anesthesia based attack on idealism. However I still find articles on anesthesia rather problematic for idealism https://neurosciencenews.com/consciousn ... oss-13009/ this article discuses anesthesia's ability of both micro and macro disconnect between firing neurons whilst this lay article discusses the dominating wave oscillation correlation to anesthetic induced unconsciousness https://www.vice.com/en/article/d3489z/ ... anesthesia
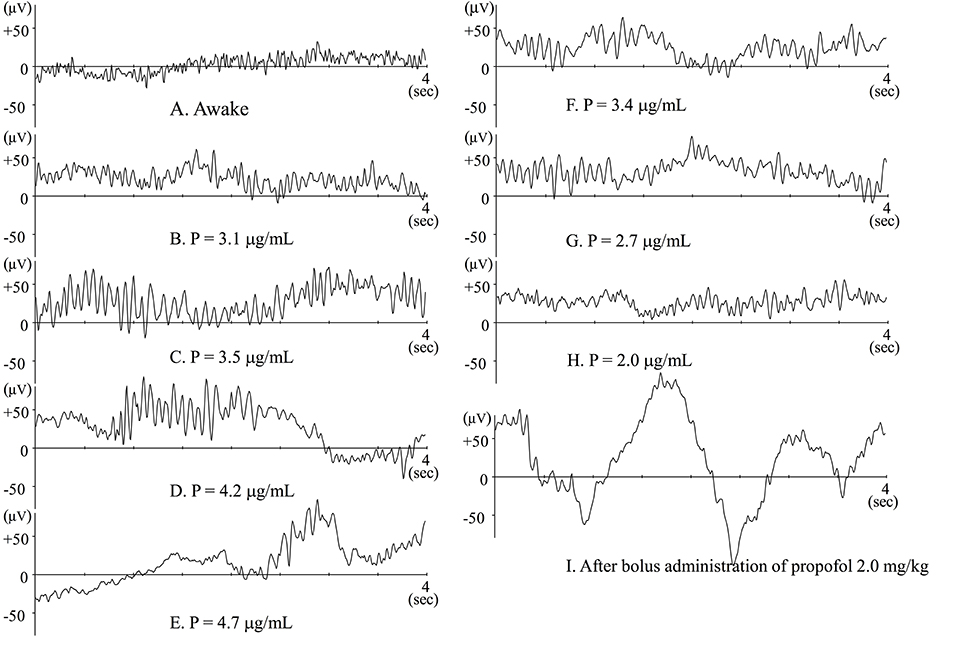
But the real debate starts here: reading this technical article https://www.frontiersin.org/articles/10 ... 00039/full in conjunction with it's figure https://www.frontiersin.org/files/Artic ... 9-g001.jpg when common anesthetic propofol is inducted slowly into a patient we are told: "When blood (and consequently effect-site) concentration of propofol slowly increases, patients are gradually sedated and finally lose responsiveness. When awake or during light sedation, EEG shows quite small and high frequency (Figure 1A). Electromyogram (EMG) contamination is often observed at this level. Just after loss of response, fast waves with small amplitude still predominate, but their frequency is slower than during wakefulness. Alpha power is quite small at this level (Figure 1B). As propofol Ce increases, EEG frequency slows and EEG amplitude becomes larger, whereupon alpha waves becomes dominant (Figure 1C). This waxing and weaning spindle wave pattern is observed during stage II of slow wave sleep. During sleep, spindles emerge only transiently, but are observed continuously during anesthesia induced by propofol or volatile anesthetics. When propofol Ce increases further, alpha waves become smaller and theta and delta waves become dominant (Figure 1D), eventually, the burst-suppression pattern emerges (Figure 1E)." However during rapid induction of Propofol or Thiopental we are told "Observation of raw EEG, however, during rapid induction is quite specific. Just after loss of response owing to bolus administration of propofol or thiopental, large delta waves emerge. At that time the BIS™ index decreases to 20–30 (Figure 1I). Similarly, during slow induction by 8% sevoflurane, similar waveforms may also be transiently observed and the BIS™ index may decrease to 10–20 (Yamaguchi et al., 2003). Soon after that, alpha or theta waves predominate and BIS™ index increases to 30–50."
Bernardo Kastrup often makes the argument that psilocybin is proof of his theory in that it lowers CBF in the brain whilst increasing phenomenal experience as we see here https://www.pnas.org/content/109/6/2138 but what of brain waves and EEG? EEG measures brain waves and said brain waves are indicative of certain brain activity https://choosemuse.com/blog/a-deep-dive ... plained-2/ in this article here https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5616440/ we are told "Psilocybin decreased the EEG spectral power in alpha frequency band, however increased the power of gamma oscillations. The LORETA analysis revealed the source of decreased alpha in midline parietal structures and occipital lobes. The increase in higher frequencies was pronounced in large temporal areas. EEG findings will be correlated with neuropsychiatric scales." This states that psilocybin INCREASES certain forms of brain activity in contrast to the CBF focused article Kastrup cites. I tried to find articles discussing CBF under anesthesia but most of the technical articles were too topic pointed and so thus I could not gleam accurate information that was consistent to make any kind of point in that regard. So is Kastrups mushroom based argument inconsistent with EEG? Is CBF more telling of brain function than EEG? I hope after careful consideration of my sources we can continue the discussion on anesthesia which I still believe is of relevance to any argument based on the primacy of consciousness. Do you believe these points challenge idealism? If not why? All quotes are from the articles listed and were written by their authors.
But the real debate starts here: reading this technical article https://www.frontiersin.org/articles/10 ... 00039/full in conjunction with it's figure https://www.frontiersin.org/files/Artic ... 9-g001.jpg when common anesthetic propofol is inducted slowly into a patient we are told: "When blood (and consequently effect-site) concentration of propofol slowly increases, patients are gradually sedated and finally lose responsiveness. When awake or during light sedation, EEG shows quite small and high frequency (Figure 1A). Electromyogram (EMG) contamination is often observed at this level. Just after loss of response, fast waves with small amplitude still predominate, but their frequency is slower than during wakefulness. Alpha power is quite small at this level (Figure 1B). As propofol Ce increases, EEG frequency slows and EEG amplitude becomes larger, whereupon alpha waves becomes dominant (Figure 1C). This waxing and weaning spindle wave pattern is observed during stage II of slow wave sleep. During sleep, spindles emerge only transiently, but are observed continuously during anesthesia induced by propofol or volatile anesthetics. When propofol Ce increases further, alpha waves become smaller and theta and delta waves become dominant (Figure 1D), eventually, the burst-suppression pattern emerges (Figure 1E)." However during rapid induction of Propofol or Thiopental we are told "Observation of raw EEG, however, during rapid induction is quite specific. Just after loss of response owing to bolus administration of propofol or thiopental, large delta waves emerge. At that time the BIS™ index decreases to 20–30 (Figure 1I). Similarly, during slow induction by 8% sevoflurane, similar waveforms may also be transiently observed and the BIS™ index may decrease to 10–20 (Yamaguchi et al., 2003). Soon after that, alpha or theta waves predominate and BIS™ index increases to 30–50."
{kind=link}
Bernardo Kastrup often makes the argument that psilocybin is proof of his theory in that it lowers CBF in the brain whilst increasing phenomenal experience as we see here https://www.pnas.org/content/109/6/2138 but what of brain waves and EEG? EEG measures brain waves and said brain waves are indicative of certain brain activity https://choosemuse.com/blog/a-deep-dive ... plained-2/ in this article here https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5616440/ we are told "Psilocybin decreased the EEG spectral power in alpha frequency band, however increased the power of gamma oscillations. The LORETA analysis revealed the source of decreased alpha in midline parietal structures and occipital lobes. The increase in higher frequencies was pronounced in large temporal areas. EEG findings will be correlated with neuropsychiatric scales." This states that psilocybin INCREASES certain forms of brain activity in contrast to the CBF focused article Kastrup cites. I tried to find articles discussing CBF under anesthesia but most of the technical articles were too topic pointed and so thus I could not gleam accurate information that was consistent to make any kind of point in that regard. So is Kastrups mushroom based argument inconsistent with EEG? Is CBF more telling of brain function than EEG? I hope after careful consideration of my sources we can continue the discussion on anesthesia which I still believe is of relevance to any argument based on the primacy of consciousness. Do you believe these points challenge idealism? If not why? All quotes are from the articles listed and were written by their authors.
{kind=link}